Food and agriculture in Ireland continue to be important sectors in terms of jobs and exports. Many of the major home grown multinationals here are in food like Glanbia and Kerry Group. Primary production in agriculture involves almost 150,000 farmers. Ireland is one of the largest dairy export nations in the world, exporting 85% of all dairy output and accounting for more than €3 billion in exports per annum. The meat sector accounts for exports of nearly €4Bn with a similar proportion of product being exported as in the dairy sector. However, food and agriculture are coming under increasing pressure. For example, the UK accounts for 40% of beef exports. Due to Brexit, the latest CSO data shows Food and Live Animal exports to the UK down 25.6% in Q12021. When this is added to current and potential trade deals with other major dairy and beef exporters such as South America, New Zealand and Australia in the near term, there will be significant and continuous pressure put on the Irish dairy and beef sectors for some time. Furthermore, the environmental impact of farming and food production is coming under greater scrutiny from consumers with a growing move to alternatives perceived as being more environmentally friendly and with less GHG emissions.
As always, the above problems are also opportunities for AgTech and FoodTech innovation and for the startups that can provide it. Over the last few years, several AgTech incubator and accelerator facilities have emerged to serve such startups. Among these are ACE in Kerry, PACE in Kilkenny and AgTechUCD. These are also associated with universities of significant expertise and early stage innovations and IP in the space that are available for licence and commercialisation. Associated universities are Munster Technological University, Waterford Institute of Technology and University College Dublin, respectively. I’d also point to Ireland’s national Food, Agriculture and AgTech research and agronomy centre, Teagasc.
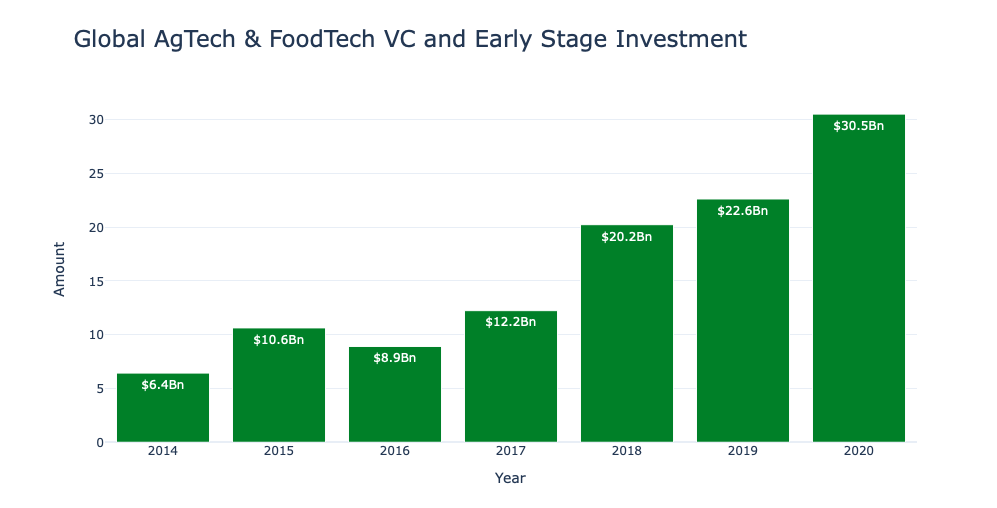
A vibrant funding environment is also needed to support emerging AgTech and FoodTech startups. Recent data shows the sector growing rapidly globally. Stock market listings for FoodTech and AgTech companies grew 8 fold in 2020, for example. Global VC investments amounted to over €30Bn in the space and have grown consistently for several years now. I’ve had a look at the seed and venture funding going into FoodTech and AgTech companies in Ireland. Looking at all Irish VC investment in 2020, which amounted to €1Bn invested in 264 companies overall, there is clear room to grow this sector in Ireland from a current 5% level of investment in AgTech and FoodTech.
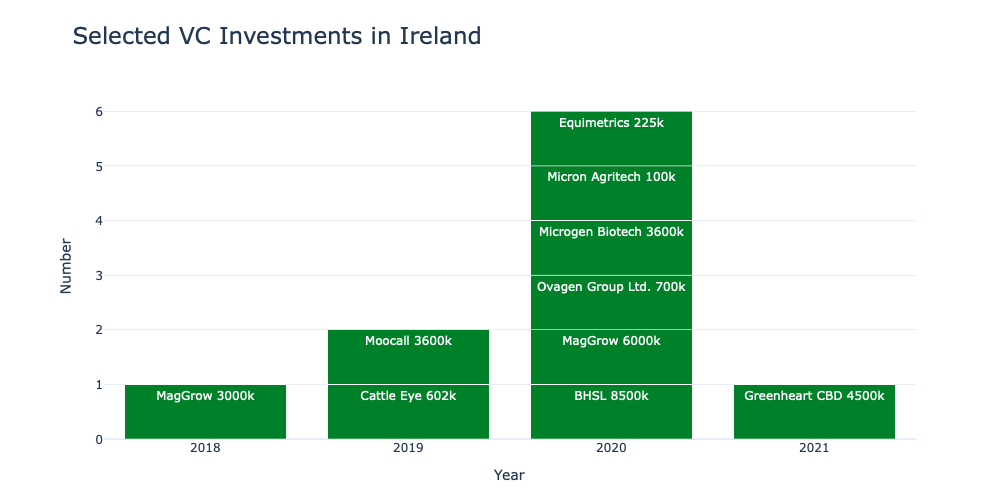
There are local VC funds such as Yield Lab and Finistere that specialise in funding startups in the AgTech and FoodTech spaces. They often co-fund in a syndicate of other private and VC investors. Looking at recent investment data in Ireland from TechIreland, there were investments in 14 AgTech companies in 2020, unchanged from the previous year. However, in contrast to 2019’s €30M invested in the sector, some €38M was invested in 2020. Where the data has been made available, the startups are active in AgriBiotech (eg. Micron Biotech) and automated animal monitoring (eg. Moocall, Cattle Eye, etc) and food products (Greenhart CBD). Considering that the specialist funds are early in their investment cycle and the growing interest being shown by privates and other funders in the space, it looks like it has room to grow.